
Partial Brachial plexus
Injury-C56 or C567
Brachial plexus injury are the injuries related to brachial plexus.
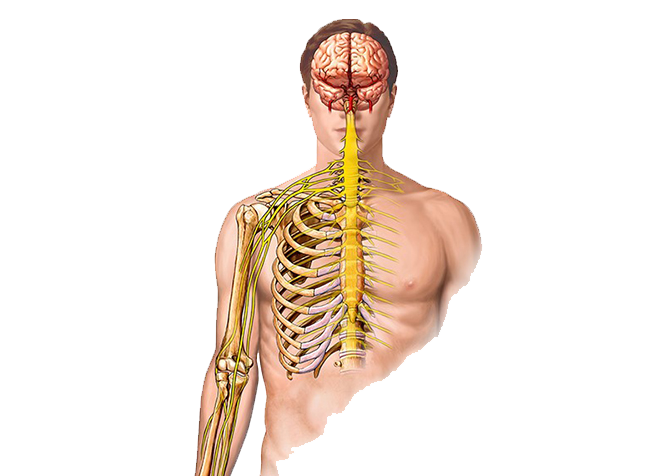
Brachial plexus injury are the injuries related to brachial plexus. Usually, partial injuries to brachial plexus occurs when the arm is forcibly stretched, pulled or injured during an accident. There is injury of C5,6 nerve roots with or without C7 nerve root in the neck causing weakness, numbness, or loss of movement in the shoulder and elbow. The hand function is good in partial brachial plexus injuries. Deficits in shoulder stability, abduction (outward movement), external and internal rotation, as well as in elbow flexion (bending of elbow) and forearm supination (rotate forearm inward) occur in partial BPI. If C7 is involved, there will also be variable weakness in extension of elbow, wrist and fingers (straightening of elbow, wrist and finger joints).

It is often seen more in men aged between 15-25 years. Upper brachial plexus (C5, C6) are more likely to stretch or rupture for their origin, whereas lower brachial plexus (C8, T1) avulse/detach from the spinal cord.
Due to very less awareness, often patient roams around and reach the right person quite late after the injury. So Plastic surgeons trained in Brachial plexus surgery are the ones who should be consulted for management of such cases. Dr Amit Agarwal specializes and have expertise of more than 11 years in the field of brachial plexus injury management and is well aware of all aspects of treatment.
It is said "sooner the treatment, better the outcome" in brachial plexus injuries. The nerves are explored, repaired and transferred during the surgery. If no recovery is seen after 3 months of accident, nerve transfer surgery is done as early as possible. Surgery can still be done for injuries within 9 months to 1 year of injury but chances of recovery would be less when compared to surgery done early at 3 months.
If nerve transfer surgery is attempted after 1 year of accident, it has been observed that chances of recovery would be very less as there's is not enough time left for nerve regeneration, so specific targeted muscle and tendon transfers are done instead of nerve transfer surgery beyond 1 year of accident.
If the patient presents to us after one year of accident and no surgery has been done for him in the past one year or no recovery is seen after the initial nerve repair, then targeted muscle and tendon transfers are done to get acceptable movements of shoulder and elbow.
After one year of accident usually no specific investigations like MR Neurography and NCV studies are done which are mandatory if the patient presents to us within one year of the accident.
Still thorough examination of the brachial plexus, muscle movements, sensory return, history of previous surgeries, ruling out of all fractures and patient's vocational abilities have to be kept in mind before proceeding for reconstruction after one year of accident.
Surgical Procedures for Complete Brachial Plexus Injuries after one year of accident
Achieving elbow flexion is one of the main major goals in reconstruction of partial brachial plexus injuries. So this is the first surgery advised to the patients when they present after one year of accident- to restore his or her elbow flexion. In this surgery muscle is taken from the thigh or back, transferred to the arm mimicking the action of biceps muscle to bring the movement of elbow flexion.
It is also done in cases where the primary nerve repair procedures have failed to yield any response even after one and a half years of the surgery.
In fewdelayed cases of more than 9 - 12 months post traumatically, even after the nerve transfer and nerve grafting techniques, within the appropriate period, functional restoration of the hand might be disappointing. For this reason, muscle transfer for elbow functionis donein addition to nerve transfer and grafting.
LD to Biceps
LD muscle is locatedin the region of the back and is usually preserved inupper arm typepartial brachial plexus injuries. It is innervated by the thoracodorsal nerve which is mostly preserved in patients with C5-6 injury. On the other hand, in C5-6–7 complete injury, LD muscle may not be available for transfer. Careful pre-operative evaluation of LD function is crucial for the success of LD transfer.
For this repair, patient is admitted, routine pre-operative investigations and pre-anesthetic checkupis doneand muscle strength of LD is confirmed. Incision is given on the side of the thorax and LD muscle is dissected free from its attachments. It is then transferred to the arm region retaining its vascular and nerve supply arising from the axilla.
Patient is kept under observation for about 7-8 days after surgery, splintage given and then discharged. Dressings changed once or twice in between and patient called for follow up after 3 weeks for suture removal. After about 6 weeks of surgery, he is advised for physiotherapy. Follow up is done every month initially for recovery, later every 3-6 months.The time period required for any elbow flexion to appear is minimum between 3 to 6 months and the complete recovery may take around one year.
Free functioning muscle transfer (For elbow flexion)
This surgery is usually done when LD muscle is weakor not working or the patient has not given the consent for harvest of muscle from his back. Then Restoration of elbow flexion is done using the reinnervated free-muscle transfer technique.
For this repair, patient is admitted and routine pre-operative investigations, pre-anesthetic checkup is done. The surgery is done under General Anaesthesia. Informed written consent form is signed before surgery. During the surgery, area of the arm and the forearm is explored for donor nerve and vessels and a tunnel is created for inset of muscle. Gracilis muscle is harvested from the thigh along with its vessels and nerve. This muscle/flap transferred to the paralysed arm and sutured. The vessels and the nerve are anastomosed under microscope by microsurgical technique.
Patient is kept under observation for about 10-12 days after surgery, free flap being monitored continuously, splintage given and then discharged. Dressings changed frequently in between, and patient called for follow up after 1week or even later. After about 1-1.5 months of surgery, once the flap is settled, patient is advised for physiotherapy, TENS therapy. Follow up is done every month initially for stability, later every 3- 6 months.
Tendon Transfer for wrist/finger extension
In cases where the hand has some function, tendon transferwill stabilize the wrist joint so as to enhance finger function and increase grip strength. It places the wrist in a stable functional position, and can improve movement and power in the elbow also.
For this repair, patient is admitted, routine pre-operative investigations and pre-anesthetic checkup is done. The surgery is done with incision on the back of the forearm, tendons are exposed and transferred to extend the wrist/fingers.Patient is kept under observation for about 2 days after surgery, splintage given and then discharged. Dressings changed once or twice in between, and patient called for follow up after 1 week for removal of sutures. For about 4-6weeks, splintage is given after surgery, patient is advised for physiotherapy to keep the distal joints supple. Follow up is done every month initially for stability, later every 3-6 months.
Trapezius transfer (for shoulder)
There is complete loss of movement of the shoulder in partial brachial plexus injuries. Partialrestoration of shoulder joint in form of abduction is possible with either shoulder joint fusion or trapezius muscle transfer.
If the patient is seen after a year of the accident, first surgery is done for restoring elbow flexion. Surgery to restore movement of the shoulder joint can be done in the second stage.Shoulder joint fusion is not very commonly tolerated by Indian patients but it is a very good procedure for patients with Partial brachial plexus injuries.
The trapezius muscle is spared because of its innervation by the spinal accessory nerve in addition to contributions from C3 and C4. However, it is also usually hypertrophied (increase in bulk) after deltoid muscle paralysis, which is why trapezius transfer is the most commonly done tendon transfer for shoulder abduction movement in adult brachial palsy.
For this repair, patient is admitted, routine pre-operative investigations and pre-anesthetic checkup is done and muscle strength is confirmed. Horizontal incision is given over the shoulder region, trapezius muscle is dissected, mobilised and brought forward and fixed to the bone in the arm. Patient is kept under observation for about 3-4 days after surgery, splintage given and then discharged. Dressings changed once or twice in between, and patient called for follow up after 2 weeks for suture removal. Once the scars are matured, after about one month of surgery, he is advised for physiotherapy. Follow up is done every month initially for recovery, later every 3-6 months.
Partial Brachial plexus Injury-C56 or C567 Images
Indivisual results may vary from person to person.
These pictures are shown for the purpose of education only.


Shaping dreams through



Know your surgeon better

Best plastic surgeon, Dr. Amit Agarwal is an American Board Certified, extensively trained, and best Plastic & Aesthetic surgeon in Lucknow. He is the Chief Plastic Surgeon heading the Department of Plastic, Microvascular, and Craniofacial surgery at Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, U.P, India. He maintains a busy practice at Avadh and Nishat Hospital and his own center - Kayakriti Plastic Surgery & Dental Center. He was formerly a Consultant in the Department of Plastic Surgery and Burns at the prestigious SGPGI, Lucknow.
MS, DNB (General Surgery) MCh, DNB (Plastic Surgery),
MNAMS, FACS, FICS, FRCS (Edinburgh, UK)
His Credentials










Three pillars of kayakriti
Privacy
We believe your experience with us should be comfortable and hassle-free to make it one of your best lifetime experiences for yours. We, here at the clinic, take full precautions to maintain your privacy in any manner. We also provide a staff who will receive you from the gate and take you to the chamber directly if you demand.
Trust
Our Surgeon is highly qualified and internationally certified with a team of skilled staff to perform any surgical or non-surgical treatment on your body.
Safety
When you plan to undergo any surgery you should always keep in mind that it's your body and it's a surgery. We, here always keep your safety a priority and will never recommend you to undergo any such procedure which is not safe for you. We also provide you with a detailed description of the complications which may occur after the surgery during the consultation as it's a surgical procedure so there may be some complications depending on the way your body reacts.
Kayakriti in news



Frequently Asked Questions
If you have flat or small breast and you want to improve your breast and hip contour ratio then you are a good candidate for it. The answer will be best provided after the first consultation with Dr Amit Agarwal.
Acute pain will be there for almost a week which gradually reduces and there will be soreness and swelling which may take up to 3 weeks to subside.
You can join your work and daily routines after a week of the procedure and can start exercising after 3 weeks of it.
Yes, you have to wear it round the clock unless we suggest you to remove it.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.














Kayakriti Plastic Surgery & Dental Center
D-43, Near Punjab National Bank, Rajajipuram, Lucknow, Uttar Pradesh - 226017, India
Phone No. +919695940009, +919695940006
Map Location

Social Media Presence