
Brachial Plexus Birth
palsy in children
an unfortunate ingury
in new born baby
Obstetric brachial plexus injury (OBPI).
Obstetric brachial plexus injury (OBPI), also known as birth brachial plexus injury (BBPI), is unfortunately a rather common injury in newborn children, incidence of 0.38 to 1.56 per 1000 live births. After birth, child with palsy is examined thoroughly by the pediatrician and parents are counseled to consult a plastic surgeon for management and any early intervention if required for palsy of arm of child. Sometimes, in villages where post birth evaluation is not possible and paralysis of arm of these children are often unnoticed initially by the parents, but when the child grows gradually and is unable to perform normal hand functions, then parents take their child to the physicia., So the patient reach the right place quite late and hence outcome is hampered. For this, a lot of awareness is required for the correct management of the impairment and to reach the right place at the right time.
Risk factors involved are large-for-gestational-age infants(big baby), multiparous pregnancies, previous deliveries resulting in brachial plexus birth palsy, prolonged labor, breech delivery(foot end of baby lower side), assisted delivery(vacuum or forceps), and difficult deliveries. Although spontaneous recovery is known, there is a large subset which does not recover and needs primary or secondary surgical intervention.
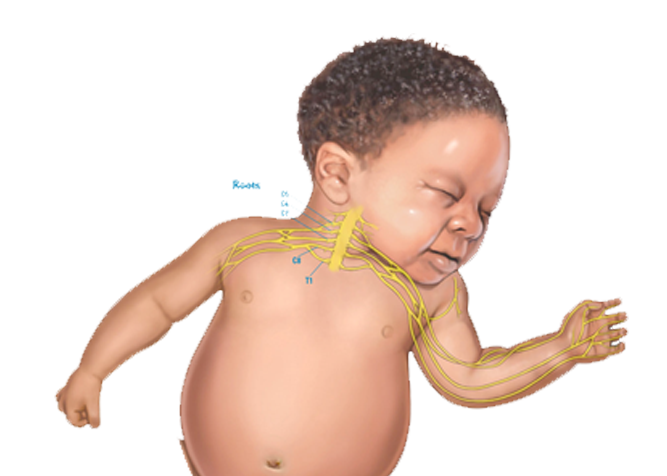
Obstetrical brachial plexus palsies are divided into two major types according to the distribution and severity of the injury:
- Upper brachial plexus palsy ("Erb's palsy"), involving the C5 and C6 nerve roots and sometimes C7 as well - In upper brachial palsy (C5 and C6 nerve roots: shoulder muscles and forearm flexors), the shoulder is held in an adducted(held towards the body), internally rotated position, while the lower arm is extended(elbow straight) and hand function remains normal. If the C7 nerve root is also involved, there is additional weakness of the triceps(it helps in straightening the elbow from inward bend position) and wrist extensor muscles(straightening the wrist from inward bend position).
- Complete brachial plexus palsy, involving all of the nerve roots from C5 to T1. - In complete brachial plexus palsy, there is complete lack of movement at the shoulder, elbow and hand with complete sensory loss as well.
Signs & Symptoms of a Brachial Plexus Birth Palsy
- Full or partial lack of movement of shoulder, elbow and hand
- A weakened hand grip
- Numbness or decreased sensation of the affected upper limb
- An odd position of the arm and hand (the arm may bend toward the body or hang)
Management Within 2 years of Birth
Most babies with a brachial plexus injury regain some or full- both movement and sensation in the affected arm. In mild cases, this might happen without treatment. Initially the concept of wait and watch was popular, to wait till the child is old enough to see all the actions properly, but that lead to delay in management and decreased outcome of any intervention done then. So now early intervention is well established and outcome is better as we see in adult patients after injury.
If the infant is brought to us within 3 months of his or her delivery with arm palsy, a clinical examination is done to assess movements of his /her shoulder, elbow and hand. If no movement is seen at the elbow at the age of 3 months then parents are counselled for a possible surgery at the age of 6 months. We do not prefer to operate and do nerve transfer surgery on infant of 3 months and prefer to wait till the child is of6 to 9 months of age.
If the infant is brought to us within a year of birth then after clinical examination nerve transfer surgery is advised. This is quite a very sensitive issue for the parents and we totally acknowledge that but it is the best option if the child has not gained any movement in his complete arm by one year of age. The results of nerve transfer surgery are quite unpredictable and different in every child and the surgery cannot guarantee how well positioned and moving arm will be after the surgery.
If the infant is brought to us between 1-2 years of birth the nerve surgery can still be attempted if the child presents within 2 years of birth. The results of repair in children is very different from their adult counterparts. The paralysis in children due to obstetric reasons is most of the times not total because of which some fibres always get reinnervated and some flicker of movements in muscles is present due to crossing of the neuromas. This innervation keeps the muscle alive and remain suitable for late nerve surgery also.
Brachial plexus birth palsy injuries are usually low velocity injuries. Most of the times, nerves ruptures or are in continuity injuries but rarely avulse. The surgery done in Nerve repair with nerve graft or nerve transfer.
Nerve repair with nerve grafts: A nerve from another area of the body, back of the foot and leg, is used to patch an injured nerve in brachial plexus.
Nerve transfer: A healthy nerve in the area or some of its fibers restores injured nerve connections. When nerve root is avulsed from spinal cord, nerve repair is not possible which is not normally seen in children due to birth palsy. Nerve transfer connects a healthy nerve outside the brachial plexus or intra-plexus functioning nerve to the nerve whose function is desired. Nerve transfer has an advantage that it permits faster reinnervation of muscle.
Upper Brachial Plexus Birth Palsy
In case of injury affecting upper brachial plexus C5–6 nerve roots, there is no movement at the shoulder and elbow joint with normal hand grip function. So to regain function of the shoulder and the elbow, nerve repair or nerve transfer surgery is done.
Brachial plexus is explored, ruptured nerves are identified, scarred portion of the nerves are removed and nerve repair is done by taking nerve graft from the leg. Incision is given in the neck region above the level of clavicle. Muscles are dissected and the nerves are explored. Neuroma Is excised and nerves are repaired by taking nerve graft from the leg if the proximal nerve roots are healthy. Additionally spinal accessory nerve is transferred to the supra scapular nerve to restore initiation of the shoulder abduction movement. This is a very vital transfer done in all children with palsy.
If proximally nerve roots are not healthy, then nerve transfers are done. Nerve transfer is a surgical option that intentionally divides a physiologically active nerve (with low donor morbidity) and transfers it to a distal more important but irreparable paralytic nerve of the brachial plexus.
In C5–6 or C5-6-7 palsy, elbow flexion is affected; however, ulnar nerve function is normal. For such case, Oberlin transfer can be of great help for the recovery of the biceps. A fascicle of the ulnar nerve is cut and sutured end to end to the nerve to biceps in the upper arm. Alternatively, biceps can be innervated through a fascicle of median nerve.
Axillary nerve is responsible for the movement of shoulder joint. Neurotization of axillary nerve can help in attaining deltoid function. In upper brachial plexus injury, radial nerve and its branch to triceps muscle are not affected. The nerve supplying one of the heads of triceps can be transferred to the axillary nerve to improve shoulder abduction. SAN to SSN transfer aids in attaining shoulder movement (infraspinatus and supraspinatus muscle function). Since isolated supraspinatus is a weak abductor, deltoid activity is also required for good abduction.
For these repairs, the child is admitted, routine pre-operative investigations and pre-anesthetic checkup is done. The child is kept under observation for about1week after surgery and then discharged. Dressings changed once or twice in between and parents are called for follow up after 1week for suture removal. After about one month of surgery, they is advised for physiotherapy. Follow up is done every month initially for recovery, later every 3months to 6 months.
The nerve regeneration occurs slowly at a rate of approximately 1 mm/day, recovery from a brachial plexus injury takes time, and parents may not experience results for several months. Parents are advised for regular physiotherapy of the child. A positive mindset and the support of family, friends, and healthcare professionals are important to recovery and rehabilitation. The results and the improvement seen in such children is much better in comparison with the injury in adults.
Global Brachial Plexus Birth Palsy
The child has no movement of the arm with complete loss of sensations incomplete brachial plexus injury.
Brachial plexus is explored, ruptured nerves are identified, scarred portion of the nerves are removed and nerve repair is done by taking nerve graft from different parts of the body. Incision is given in the neck region above the level of clavicle. Muscles are dissected and the nerves are explored. Neuroma Is excised and nerves are repaired by taking nerve graft from the leg if the proximal nerve roots are healthy. Additionally spinal accessory nerve is transferred to the supra scapular nerve to restore initiation of the shoulder abduction movement. This is a very vital transfer done in all children with global palsy.
In global palsy, if proximal nerve roots are not healthy and local nerve transfers are unavailable most of the time so extra-plexus nerve transfer like intercostal nerve transfers or C4 transfer are preferred. The commonly used nerve transfers target to improve shoulder abduction, elbow flexion, elbow extension, finger flexion and sensory function of the handin a child.
Various extra-plexus sources like spinal accessory nerve (SAN), intercostal nerves, cervical plexus can be used for nerve transfer.
For these repairs, the child is admitted, routine pre-operative investigations and pre-anesthetic checkup is done. The child is kept under observation for about1week after surgery and then discharged. Dressings changed once or twice in between and parents are called for follow up after 1week for suture removal. After about one month of surgery, they is advised for physiotherapy. Follow up is done every month initially for recovery, later every 3months to 6 months.
The nerve regeneration occurs slowly at a rate of approximately 1 mm/day, recovery from a brachial plexus injury takes time, and parents may not experience results for several months. Parents are advised for regular physiotherapy of the child. A positive mindset and the support of family, friends, and healthcare professionals are important to recovery and rehabilitation. The results and the improvement seen in such children is much better in comparison with the injury in adults
Late presentation of Brachial Plexus Birth Palsy
If the child is brought to us late after 2 years of birth, then the results of nerve transfer surgery are not good and fruitful. The child is allowed to grow and the child is closely evaluated at an interval of3 to 6 months regularly and any signs of recovery monitored. The child will eventually get few movements back in his arm, forearm and hand but will have multiple residual deformities due to cross innervation to different muscles which would require attention and surgeries in his/her life during growing years.
Parents are advised for regular physiotherapy of the child. A positive mindset and the support of family, friends, and healthcare professionals are important to recovery and rehabilitation. The results and the improvement seen in such children is much better in comparison with the injury in adults.
Brachial plexus birth palsy injuries are usually low velocity injuries. Most of the times, nerves ruptures or are in continuity injuries but rarely avulse. The distance of separation of the injured nerve ends is small in children after trauma during birth and hence reinnervation occur leading to misdirected cross innervation of fibres. This result in inadequate recovery of muscles and co-contractions. Some muscle groups recover earlier than their antagonists and unopposed action of these muscles combined with co-contractions could result in no action at the joints and contractures.
Results is- inadequate functional range of moments and deformities at various joints which are initially correctable but can lead to fixed contractures if not corrected.
A) Shoulder deformities
If there is less movement of shoulder outward (abduction)- If the muscles responsible for adduction of the arm are tight and the muscle responsible for movement of the shoulder outwards are intact, then surgical release of these tight muscles will help. If the muscles responsible for the movement of shoulder outwards are paralysed, then trapezius muscle transfer is done.If there is less movement of lateral rotation of the shoulder- The most common procedure done is the transfer of LD muscle which is situated at the back to the muscle responsible for rotating the shoulder externally.If both abduction and external rotation of the shoulder are less- Combination of both the procedures mentioned above are donein stages.
B) Elbow flexion deformity - which can be corrected by serial casting of the joint.
C) Forearm deformities - which can be eithersupination deformityor pronation deformity. These deformities can be corrected by rerouting of specific muscles and osteotomies.
D) Hand deformities - loss of wrist extension These hand deformities can be corrected by tendon transfers
E) Other deformities - There could be other deformities as well in a child which can be corrected as per the requirement
Brachial Plexus Birth palsy in children Images
Indivisual results may vary from person to person.
These pictures are shown for the purpose of education only.


Shaping dreams through



Know your surgeon better

Best plastic surgeon, Dr. Amit Agarwal is an American Board Certified, extensively trained, and best Plastic & Aesthetic surgeon in Lucknow. He is the Chief Plastic Surgeon heading the Department of Plastic, Microvascular, and Craniofacial surgery at Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, U.P, India. He maintains a busy practice at Avadh and Nishat Hospital and his own center - Kayakriti Plastic Surgery & Dental Center. He was formerly a Consultant in the Department of Plastic Surgery and Burns at the prestigious SGPGI, Lucknow.
MS, DNB (General Surgery) MCh, DNB (Plastic Surgery),
MNAMS, FACS, FICS, FRCS (Edinburgh, UK)
His Credentials










Three pillars of kayakriti
Privacy
We believe your experience with us should be comfortable and hassle-free to make it one of your best lifetime experiences for yours. We, here at the clinic, take full precautions to maintain your privacy in any manner. We also provide a staff who will receive you from the gate and take you to the chamber directly if you demand.
Trust
Our Surgeon is highly qualified and internationally certified with a team of skilled staff to perform any surgical or non-surgical treatment on your body.
Safety
When you plan to undergo any surgery you should always keep in mind that it's your body and it's a surgery. We, here always keep your safety a priority and will never recommend you to undergo any such procedure which is not safe for you. We also provide you with a detailed description of the complications which may occur after the surgery during the consultation as it's a surgical procedure so there may be some complications depending on the way your body reacts.
Kayakriti in news



Frequently Asked Questions
If you have flat or small breast and you want to improve your breast and hip contour ratio then you are a good candidate for it. The answer will be best provided after the first consultation with Dr Amit Agarwal.
Acute pain will be there for almost a week which gradually reduces and there will be soreness and swelling which may take up to 3 weeks to subside.
You can join your work and daily routines after a week of the procedure and can start exercising after 3 weeks of it.
Yes, you have to wear it round the clock unless we suggest you to remove it.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.














Kayakriti Plastic Surgery & Dental Center
D-43, Near Punjab National Bank, Rajajipuram, Lucknow, Uttar Pradesh - 226017, India
Phone No. +919695940009, +919695940006
Map Location

Social Media Presence