
Complete Brachial plexus
Injury-C5678T1
Brachial plexus injury are the injuries related to brachial plexus.
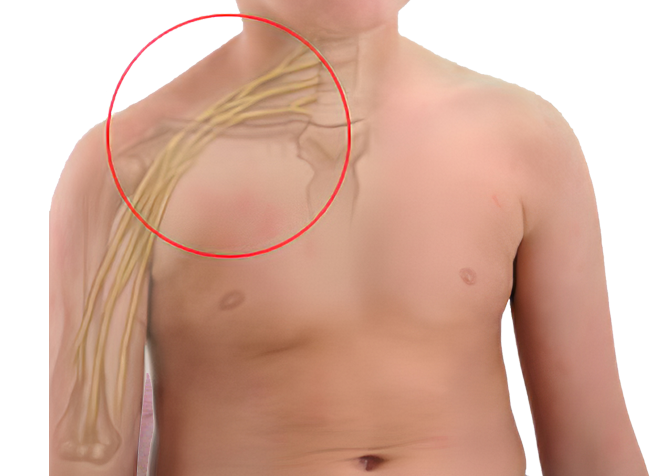
Brachial plexus injury are the injuries related to brachial plexus. Usually,complete injuries to brachial plexus occurs when the arm is forcibly stretched, pulled or injured during an accident.There is complete transection of C5,6,7,8 and T1 nerve roots in the neck causing weakness, numbness or loss of movement in the shoulder, arm, forearm and hand. The limb is completely dead in Pan/complete brachial plexus injuries. He/she is unable to lift their hand from the shoulderandelbow and wrist joint, lose all movements at all joints and hand grip with inability to hold objects and feel sensation in that limb. It is often seen more in men aged between 15-25 years. Upper brachial plexus (C5, C6) are more likely to stretch or rupture for their origin, whereas lower brachial plexus(C8, T1) avulse/detach from the spinal cord.

Examination of Brachial Plexus Injury
- Immediately after the accident due to any reason, patient must be thoroughly examined to rule out any fracture at the site of injury or injury to other parts of body, such as head, spinal cord or chest injury.
- Level of consciousness of the patient after the accident should be enquired for and whether he/she was able/not able to lift his limb after accident and had/ had not any sensation then, which can be a clue for planning management later.
Due to very less awareness, often patient roams around and reach the right person quite late after the injury. So Plastic surgeons trained in Brachial plexus surgery are the ones who should be consulted for management of such cases. Dr Amit Agarwal specializes and have expertise of more than 11 years in the field of brachial plexus injury management and is well aware of all aspects of treatment.
After patient has recovered from the other injuries, patient will be advised for regular physiotherapy and, explained to examine himself as per the features described below and follow up is done every month. If no recovery is perceived, patient will undergo few diagnostic investigation. Chest radiographs, Magnetic Resonance Neurography of Brachial Plexus, Pulmonary function tests (PFT), Electromyelography (EMG) and Nerve Conduction Studies (NCSs) are done to confirm the diagnosis, localize and characterize the nerve lesion.
Timing of surgery in Brachial Plexus injury
Next important factor is time interval between the accident and surgical intervention. It is said "sooner the treatment, better the outcome" in brachial plexus injuries. The nerves are explored, repaired and transferred during the surgery. In case of sharp open injury, immediate surgery is performed, and zone of damage is explored/identified. Otherwise in blunt closed injuries which are more common,observation is done for the first 2-3 months, which gives the time for any spontaneous recovery and if present, we can wait for further 3 months. If no recovery is seen after 3 months of accident, nerve transfer surgery is done as early as possible. Surgery can still be done for injurieswithin9 months to 1 year of injury but chances of recovery would be less when compared to surgery done early at 3 months.
If nerve transfer surgery is attempted after 1 year of accident, it has been observed that chances of recovery would be very less as there's is not enough time left for nerve regeneration, sospecific targeted muscle and tendon transfersare done instead of nerve transfer surgery beyond 1 year of accident.
The maximum result which a patient with full effort and physiotherapy gets in complete brachial plexus injury is that he is able to abduct (lift his arm away from the body) upto 90 degrees, flex the elbow (bend elbow towards the body) and mild grip in hand (just to hold any object). So that he can use his paralyzed hand as a supportive hand.
SurgicalProcedure of Nerve Repair/ Transfer for Complete BPI
The surgery is done under General Anaesthesia and patient is admitted a day before surgery in the hospital. Routine blood investigations are done, Pre-anaesthetic checkup is done, and Informed written consent form is signed before surgery. In most of the cases, nerve is also harvested from the leg for repair of complete brachial plexusinjuries.It does not create any deficit in the leg apart from mild sensory abnormality in the outer aspect of the ankle region which subsides overtime.
The procedure is best done within a golden time period, within 3-5 months of the injury, to reactivate the paralyzed muscle(s) early, effectively, and successfully tomuscle strength to grade 4 power.
Nerve repair
Nerve repair is done in cases of rupture of nerves. Brachial plexus is explored, ruptured nerves are identified, scarred portion of the nerves are removed and nerve repair is done by taking nerve graft from different parts of the body. Usually, Nerve repair is possible in upper brachial plexus rupture as the lower trunks are avulsed from the spinal cord making nerve repairs impossible. Incision is given in the neck region above the level of clavicle. Muscles are dissected and the nerves are explored. Neuroma Is excised from the upper brachial plexus andnerves are repairedby taking nerve graft from the leg if the proximal nerve roots are healthy.
Additionally spinal accessory nerve is transferred to the supra scapular nerve torestore initiation of the shoulder abduction movement. This is a very vital transfer done in all Brachial Plexus Injuries.
Nerve Transfer
Nerve transfer is a surgical option that intentionally divides a physiologically active nerve (with low donor morbidity) and transfers it to a distal more important but irreparable paralytic nerve of the brachial plexus.
- Intraplexus (within the plexus) Nerve Transfer
Usually,Intraplexus nerve transfer is applicable in cases of avulsionofnerve from the spinal cord, in which at least one of the spinal nerves is a rupture injury and still available for transfer—not to its original pathway, but to other more important nerves. Intraplexus nerve transfer is individualized depending upon the intraoperative findings, the surgeon's philosophy, and the patient's condition and requirements - Extraplexus(outside the plexus) Nerve transfer
Extraplexusnerve transfer involves the transfer of a neighbouring nerve (from the same side or opposite neck) to the avulsed brachial plexus for the neurotization of a paralytic nerve. The reported donor nerves in common use are mostly aimed at motor re-innervation. These include the- phrenic (Ph) nerve,
- spinal accessory (XI) nerve (accessed by an anterior neck approach),
- deep motor branches of the cervical plexus (cervical motor branches; CMBs), hypoglossal nerve (XII), and the
- contralateral C7 (CC7) spinal nerve
- intercostal nerves.
- Extraplexus sensory nerve transfer, such as supraclavicular sensory nerves to the median nerve transfer, is sometimes used to provide sensation to the paralytic hand.
Recovery after Brachial Plexus surgery
Brachial plexus neurotisation procedure is a long surgery and usually takes about 6 to 8 hours minimum. After the surgery the patient is usually kept in the hospital for 2 days and is allowed to go home thereafter. The sutures are non dissolvable and are removed on 14 days. After that regular monthly follow up examination is mandatory to assess the progress of the repair and nerve regeneration.
The nerve regeneration occurs slowly at a rate of approximately 1 mm/day, recovery from a brachial plexus injury takes time, and patients may not experience results for several months even after successful surgery.
Patient is advised for regular physiotherapy, TENS therapy (transcutaneous electric nerve stimulation) after the surgery.
A positive mindset and the support of family, friends, and healthcare professionals are important to recovery and rehabilitation
The result of complete brachial plexus injuries repair is quite unpredictable and in the best of hands is around 60 to 70%. The patients may require additional surgeries in future alsoto target these specific functions which the patient wants to regain in his/her arm.
Complete Brachial plexus Injury-C5678T1Images
Indivisual results may vary from person to person.
These pictures are shown for the purpose of education only.


Shaping dreams through



Know your surgeon better

Best plastic surgeon, Dr. Amit Agarwal is an American Board Certified, extensively trained, and best Plastic & Aesthetic surgeon in Lucknow. He is the Chief Plastic Surgeon heading the Department of Plastic, Microvascular, and Craniofacial surgery at Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, U.P, India. He maintains a busy practice at Avadh and Nishat Hospital and his own center - Kayakriti Plastic Surgery & Dental Center. He was formerly a Consultant in the Department of Plastic Surgery and Burns at the prestigious SGPGI, Lucknow.
MS, DNB (General Surgery) MCh, DNB (Plastic Surgery),
MNAMS, FACS, FICS, FRCS (Edinburgh, UK)
His Credentials










Three pillars of kayakriti
Privacy
We believe your experience with us should be comfortable and hassle-free to make it one of your best lifetime experiences for yours. We, here at the clinic, take full precautions to maintain your privacy in any manner. We also provide a staff who will receive you from the gate and take you to the chamber directly if you demand.
Trust
Our Surgeon is highly qualified and internationally certified with a team of skilled staff to perform any surgical or non-surgical treatment on your body.
Safety
When you plan to undergo any surgery you should always keep in mind that it's your body and it's a surgery. We, here always keep your safety a priority and will never recommend you to undergo any such procedure which is not safe for you. We also provide you with a detailed description of the complications which may occur after the surgery during the consultation as it's a surgical procedure so there may be some complications depending on the way your body reacts.
Kayakriti in news



Frequently Asked Questions
If you have flat or small breast and you want to improve your breast and hip contour ratio then you are a good candidate for it. The answer will be best provided after the first consultation with Dr Amit Agarwal.
Acute pain will be there for almost a week which gradually reduces and there will be soreness and swelling which may take up to 3 weeks to subside.
You can join your work and daily routines after a week of the procedure and can start exercising after 3 weeks of it.
Yes, you have to wear it round the clock unless we suggest you to remove it.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.
This surgery does not affect the ducts or the areas of the breast involved in milk production. Thus, it does not affect the breast feeding.














Kayakriti Plastic Surgery & Dental Center
D-43, Near Punjab National Bank, Rajajipuram, Lucknow, Uttar Pradesh - 226017, India
Phone No. +919695940009, +919695940006
Map Location

Social Media Presence